Are you in a caring profession? If so, do you ever feel preoccupied with the suffering of the people you work with?
In a helping role, we get up close with the trauma and suffering of clients and patients to try to understand their perspective and resonate with their pain.
Compassion is a wonderful gift to those we help. It is the experience of deep empathy for a person suffering coupled with a desire to resolve their misfortune or remedy their pain (Figley, 2002b; Stamm, 2002).
Although compassion can be deeply rewarding, it can also come at a cost, particularly if we’re frequently exposed to others’ traumatic experiences in our role as helpers.
In this article, we’ll outline some symptoms of compassion fatigue, delve into how it begins, and provide real-life examples of compassion fatigue in the helping profession.
Compassion fatigue is a form of stress or tension that arises from frequent contact with traumatized people, where we become preoccupied with the suffering or pain of others (Hunsaker, Chen, Maughan, & Heaston, 2015).
Compassion fatigue is a serious problem that can undermine a person’s mental and physical health and negatively affect their relationships and ability to care for others (Cocker & Joss, 2016).
Compassion fatigue can show itself in a range of symptoms and behaviors, such as:
Diminished ability or interest to care for others
Preoccupation with people you help
Mental and/or physical exhaustion
Anger and irritability
Anxiety and/or depression
Intrusive thoughts
Sleep problems
Being easily startled
Hopelessness about helping work
Flashbacks
Hypervigilance
Avoidance of certain activities, situations, or people you help
Feeling like a failure as a helper
Drops in productivity
Emotional numbness
Trouble separating personal and professional life
A decreased capacity to experience sympathy and empathy
Dysfunctional coping behaviors, e.g., misusing alcohol or drugs
Taking more time off work
Reduced decision-making ability
Feeling disconnected
Decreased satisfaction or enjoyment with work (Cocker & Joss, 2016; Clay, 2020; Stamm, 2010)
Compassion fatigue vs empathy fatigue
The terms compassion fatigue and empathy fatigue are occasionally used interchangeably. But this can confuse the issue slightly, as some models of compassion fatigue don’t agree on the role of empathy in the development of compassion fatigue.
According to Figley (2002a), without the ability to empathize, there is little room for compassion fatigue, because empathy is essential to helping work and experiencing the strains of caring. Empathic concern is our impetus to help those people that are suffering, for example, by providing our services as a therapist (Figley, 2002a).
Our empathic response toward clients and patients is how we try to remedy a client’s suffering and can lead us to share in their emotional responses. “Compassion stress” is the consequence of empathic responding and represents the ongoing desire to reduce the suffering of the client or patient (Figley, 2002a).
If compassion stress is severe and/or compounded by other life stresses, it can lead to compassion fatigue (Figley, 2002a), which can be emotionally overwhelming and make it more difficult to experience empathy (Clay, 2020).
However, a more recent model of compassion fatigue challenges the idea that it is empathy that makes us vulnerable to compassion fatigue (Coetzee & Laschinger, 2017). Instead, Coetzee and Laschinger (2017) suggest a lack of resources, the person’s response to the distress, and inadequate positive feedback make us susceptible to compassion fatigue. We’ll get into these models in more detail a little further on.
What Causes Compassion Fatigue?
There are two components to compassion fatigue: secondary traumatic stress and burnout.
When our job is to help others who are in distress or traumatized, we must adopt the perspective of the person who is suffering to empathize with them (Figley, 2002a).
By doing this, we are necessarily exposed to the emotional energy and trauma of the particular patient we are working with, which can lead to secondary traumatic stress (Figley, 2002b; Stamm, 2012).
Over time, we can also experience burnout and feel as though our helping work is not having a positive impact ( Stamm, 2012).
So, why do we continue to do compassionate work if it costs us?
According to Stamm (2012), we do it for compassion satisfaction – the positive and pleasurable experience of helping others that can be nourishing. You can experience compassion satisfaction and fatigue simultaneously, but when compassion fatigue overrides, it may undermine your ability to feel compassion satisfaction (Stamm, 2002; Bride, Radey, & Figley, 2007).
Burnout and secondary traumatic stress are both components of compassion fatigue, but these constructs are distinct from each other (Stamm, 2012; Cocker & Joss, 2016).
When we’ve been stressed for a long time, we can reach a state of physical, mental, and emotional exhaustion: burnout (National Health Service, n.d.). Burnout may have a range of causes, and it does not happen specifically after being exposed to another person’s trauma (Figley, 2002a; Middleton, 2015).
In contrast, secondary traumatic stress occurs when we’re unable to save someone from their suffering, and we become distressed and preoccupied with their pain (Cocker & Joss, 2016). The symptoms of secondary trauma can look very similar to post-traumatic stress disorder (Middleton, 2015).
Burnout builds up and takes hold gradually. The experience of secondary traumatic stress is typically fast, but it can contribute to the experience of burnout (Middleton, 2015; Stamm, 2012).
3 Real-Life Examples of Compassion Fatigue
Anyone in a helping role could develop compassion fatigue, particularly if your compassion satisfaction is dwindling or you’re not getting enough support at work.
Nursing
Nursing requires huge amounts of compassion and empathy to support those in pain, and although it can be extremely rewarding, it can also be a very emotionally demanding role.
One study found a greater distance between the care the nurses were able to provide and the quality of care they wanted to provide, as well as other physical and emotional stresses that made compassion fatigue worse (Perry, Toffner, Merrick, & Dalton, 2011). Work–life balance, colleague support, and acknowledgment were some factors that helped reduce it (Perry et al., 2011).
Low levels of manager support have predicted higher levels of burnout and compassion fatigue among emergency department nurses, whereas high levels of manager support contributed to greater compassion satisfaction (Hunsaker et al., 2015).
Social workers
Social workers frequently provide help to people who have experienced trauma, such as survivors of domestic violence or abuse. Following the September 11 terrorist attacks on the World Trade Center, researchers found that New York social workers who were exposed to clients who had been traumatized experienced secondary trauma themselves (Adams, Figley, & Boscarino, 2008).
Another study exploring the experiences of compassion fatigue among six social workers found that effective supervision and a supportive work environment played an important role in enhancing the social workers’ resilience (Kapoulitsas & Corcoran, 2015).
Foster carers
The role of foster carers is to offer children in public care a safe and loving home, and foster carers are often exposed to the early traumatic experiences of the children they look after (Bridger, Binder, & Kellezi, 2020).
A survey involving 187 British foster carers found high levels of burnout and secondary traumatic stress among the carers. Foster carers provide round-the-clock care, and not getting enough time off or away from caring was a consistent issue raised by the carers (Bridger et al., 2020).
Drowning in empathy: the cost of vicarious trauma
Fascinating Research Findings & Models
Many models of compassion fatigue have been developed over the years, but one of the most influential was the Compassion Stress and Fatigue Model by Figley (1995, 2002a, 2002b).
The Compassion Stress and Fatigue Model
At the heart of it, Figley (1995, 2002a) proposes that empathy and emotional energy are essential for therapists (or helpers) to connect with others and to respond to their suffering effectively. Essentially, we need to be able to adopt the perspective of the person we’re helping to understand the best way to help them.
As a result, therapists are then directly exposed to the emotions of the person in pain and are motivated to remedy or decrease their suffering through their empathetic responses (Figley, 2002a).
When the therapist feels a continuing demand to reduce the client’s suffering, this can create compassion stress. This can negatively impact the therapist’s wellbeing unless they manage this stress through a sense of achievement or disengagement (Figley, 2002a).
With disengagement, the therapist actively distances themselves from the client’s suffering between sessions and puts effort into their own self-care. Obtaining a sense of achievement and satisfaction from helping work also requires therapists to have some awareness to understand the limits of their responsibility (Figley, 2002a).
A few other important factors that contribute to compassion fatigue include (Figley, 2002a):
Prolonged exposure
The feeling of responsibility for helping those in pain for a significant period of time—breaks and vacations are important to avoid this.
Traumatic recollections
Emotional memories that the client triggers for the therapist—these may reflect the therapist’s experiences of other clients who were especially difficult, demanding, or suffering greatly.
Life disruption
Any life event that disrupts your routine, schedule, or ability to manage and cope with your daily responsibilities.
Compassion Fatigue Model
The compassion fatigue model (Coetzee & Laschinger, 2017) aimed to build on previous models of compassion fatigue by weaving in the conservation of resources theory and growing research on the social neuroscience of empathy.
Ultimately, this model suggests that positive feedback, balanced resources, and reducing self-focused personal distress when working with those we help can mitigate compassion fatigue (Coetzee & Laschinger, 2017).
– Resources
The conservation of resources theory proposes that all caregivers have a certain balance of resources. The caregiver’s resource balance can be healthy or diminished for many reasons; for instance, they may have poor resources in their workplace, a lack of support at home, or low emotional energy (Coetzee & Laschinger, 2017).
– Resource appraisal
Your assessment of your resource balance will influence whether or not you see those you help as a threat to your resources and can influence whether your empathic focus is on yourself or the client (Coetzee & Laschinger, 2017).
– Other focus
Adopting an other focus means we are empathizing with the client and see things from their viewpoint, while also knowing that there is a clear boundary between the self and the other (Coetzee & Laschinger, 2017).
When investing resources in helping others, Coetzee and Laschinger (2017) suggest that therapists will expect some resource gain from helping in the form of positive feedback, such as the outcome for the client or praise. If the therapist faces a negative outcome, such as a lack of recognition or failed treatment, this can lead to a sense of resource loss (Coetzee & Laschinger, 2017).
– Self-focus
The main difference between other- and self-focus is the lack of distinction between the self and other. Self-focus can lead to more distress for the therapist.
Self-focused propositional processing (controlled, voluntary, and “cognitive”) can lead the therapist to assess their own thoughts and feelings about the client and their suffering, which can sometimes be helpful and other times, lead to distress (Coetzee & Laschinger, 2017).
Self-focused experiential processing (automatic, involuntary, and associated with emotional resonance) is more problematic and can lead to distress for the therapist and motivate them to avoid or withdraw from the client (Coetzee & Laschinger, 2017).
Overcoming Compassion Fatigue
How do we overcome compassion fatigue? With self-care and self-compassion.
While a hallmark of therapist-practitioner relationships is compassion, practitioners often fail to apply it to themselves (Coaston, 2017).
Therefore, an essential first step in overcoming compassion fatigue is tending to the self with kindness.
Being compassionate to the self might mean setting emotional boundaries, reducing one’s workload, letting colleagues know that we’re struggling, and even seeking professional help. Although it is difficult to be kind to ourselves when our clients need us, we know that we can’t be the best support if we feel vulnerable.
In saying this, overcoming compassion fatigue isn’t always about making massive changes. Sometimes simply connecting to our values of why we do this work can be crucial in combating and preventing compassion fatigue.
Compassion fatigue interventions
As well as getting enough support at work and enhancing opportunities for compassion satisfaction, some simple interventions may be helpful to reduce compassion fatigue.
– Trauma training
Specialized trauma training has been linked to lower compassion fatigue and higher compassion satisfaction, suggesting that being more knowledgeable about trauma may be a helpful buffer against trauma exposure (Sprang, Clark, & Whitt-Woosley, 2007).
– Self-care
This may seem like an obvious one, but it’s something many of us find hard to prioritize when caring for others. One study of hospice professionals found that those reporting a greater number of self-care strategies experienced lower burnout and compassion fatigue (Alkema, Linton, & Davies, 2008).
– Mindfulness
Research has found a positive relationship between mindfulness (attention awareness) and compassion satisfaction, and a negative relationship between mindfulness and secondary traumatic stress and burnout in people supporting the traumatically bereaved (Thieleman & Cacciatore, 2014).
The Psychology of Vicarious Trauma
We are vulnerable to secondary traumatic stress (compassion fatigue) and vicarious traumatization when working with trauma survivors (Jenkins & Baird, 2002).
But vicarious trauma is different from compassion fatigue and involves the changing of the helper’s schemas (mental frameworks or life beliefs) because of exposure to the traumatic experiences of others (Jenkins & Baird, 2002).
Learning about the trauma of others can trigger profound shifts in how a helper understands themselves or others, which can be very distressing (Jenkins & Baird, 2002).
Compared to secondary traumatic stress, vicarious trauma is less observable, happening below the surface, as the helper’s worldview is transformed. But distress and burnout symptoms can be common to both experiences (Jenkins & Baird, 2002).
As with secondary traumatic stress, vicarious trauma happens through empathic engagement with someone else’s trauma. But while secondary traumatic stress often happens rapidly, vicarious trauma builds up over time through repeatedly hearing about other people’s trauma (Jenkins & Baird, 2002).
3 Best Books on the Topic
Compassion fatigue is a complex and fascinating topic that is highly relevant to anyone in a caring role. If you’re keen to expand your library with compassion fatigue literature, here are some of our top picks:
1. Treating Compassion Fatigue – Charles R. Figley
Figley is one of the pioneers of traumatology research and theory, and this book is an extremely informative and comprehensive read for any trauma practitioner.
An impressive list of traumatology researchers have contributed to the book’s 11 chapters, which cover compassion fatigue theory, research, and treatment.
2. Help for the Helper: The Psychophysiology of Compassion Fatigue and Vicarious Trauma – Babette Rothschild
This book delves into the psychophysiology of compassion fatigue and vicarious trauma and explores neurobiology, social psychology, folk psychology, and strategies for managing stress and burnout.
Rothschild is an internationally acclaimed expert in the treatment of trauma and a body-psychotherapist, and she has written numerous books, including the widely popular The Body Remembers series.
3. Surviving Compassion Fatigue: Help for Those Who Help Others – Beverly D. Kyer
Kyer is a clinical social worker and trauma specialist who has dedicated much of her life to helping others.
In this book, you’ll learn about her personal experience with compassion fatigue and how she overcame it.
This book has great practical appeal, as you’ll learn strategies and techniques to support your wellbeing and self-care while caring for those in need.
We all need a little help with self-care from time to time, and if you’re overdue for some time-out or time-off, take this as your cue to prioritize yourself. Below are some of our free self-care resources to help you get started.
Self-Care Check-In This self-assessment uses ratings and reflection questions to help you determine how to better meet your self-care needs.
Self-Care Checkup This worksheet helps you consider the frequency and quality of your self-care across five important life domains and includes a useful list of more than 40 self-care activities.
My Self-Care Promise This worksheet helps you reflect on your unique needs, identify activities you find restorative, and promise to treat yourself kindly when self-care is needed.
If you’re looking for more science-based ways to help others manage stress without spending hours on research and session prep, this collection contains 17 validated stress management tools for practitioners. Use them to help others identify signs of burnout and create more balance in their lives.
Help your clients prevent burnout, handle stressors, and achieve a healthy, sustainable work-life balance with these 17 Stress & Burnout Prevention Exercises [PDF].
Many of us pursuing a career in the helping profession find great joy, meaning, and fulfillment in helping others.
But at the same time, offering compassion to those in need is a deeply emotional and resource-demanding process. Compassion fatigue comes in the form of secondary traumatic stress and burnout and can happen when being exposed to other people’s trauma.
Compassion satisfaction is a truly nourishing and pleasant experience that comes from helping others, which may help to stave off compassion fatigue. Having adequate resources to do your job and a supportive work environment, managing self-related distress, receiving positive feedback, and practicing self-care are other key factors that may help to reduce compassion fatigue.
Compassion fatigue can affect your mental and physical wellbeing and your ability to care for others. If you’re concerned that you may be developing compassion fatigue, it’s important to speak to someone and ask for support. As well as caring for others, you need to care for yourself too.
Adams, R. E., Figley, C. R., & Boscarino, J. A. (2008). The compassion fatigue scale: Its use with social workers following urban disaster. Research on Social Work Practice, 18(3), 238–250.
Alkema, K., Linton, J. M., & Davies, R. (2008). A study of the relationship between self-care, compassion satisfaction, compassion fatigue, and burnout among hospice professionals. Journal of Social Work in End-of-Life & Palliative Care, 4(2), 101–119.
Bride, B. E., Radey, M., & Figley, C. R. (2007). Measuring compassion fatigue. Clinical Social Work Journal, 35(3), 155–163.
Bridger, K. M., Binder, J. F., & Kellezi, B. (2020). Secondary traumatic stress in foster carers: Risk factors and implications for intervention. Journal of Child and Family Studies, 29(2), 482–492.
Clay, R. A. (2020, June 11). Are you experiencing compassion fatigue? American Psychological Association. Retrieved from https://www.apa.org/topics/covid-19/compassion-fatigue
Coaston, S. C. (2017). Self-care through self-compassion: A balm for burnout. Professional Counselor, 7(3), 285-297.
Cocker, F., & Joss, N. (2016). Compassion fatigue among healthcare, emergency and community service workers: A systematic review. International Journal of Environmental Research and Public Health, 13(6), 618.
Coetzee, S. K., & Laschinger, H. K. (2017). Toward a comprehensive, theoretical model of compassion fatigue: An integrative literature review. Nursing & Health Sciences, 20, 4–15.
Figley, C. R. (Ed.). (1995). Compassion fatigue: Coping with secondary traumatic stress disorder in those who treat the traumatized. Brunner/Mazel.
Figley, C. R. (2002a). Compassion fatigue: Psychotherapists’ chronic lack of self care. Journal of Clinical Psychology, 58(11), 1433–1441.
Figley, C. R. (2002b). Treating compassion fatigue. Brunner/Rutledge.
Hunsaker, S., Chen, H. C., Maughan, D., & Heaston, S. (2015). Factors that influence the development of compassion fatigue, burnout, and compassion satisfaction in emergency department nurses. Journal of Nursing Scholarship, 47(2), 186–194.
Jenkins, S. R., & Baird, S. (2002). Secondary traumatic stress and vicarious trauma: A validational study. Journal of Traumatic Stress, 15(5), 423–432.
Kapoulitsas, M., & Corcoran, T. (2015). Compassion fatigue and resilience: A qualitative analysis of social work practice. Qualitative Social Work, 14(1), 86–101.
Kyer, B. D. (2016). Surviving compassion fatigue: Help for those who help others. Gatekeeper Press.
Middleton, J. (2015). Addressing secondary trauma and compassion fatigue in work with older veterans: An ethical imperative. Journal of Aging Life Care, 5, 1–8.
National Health Service. (n.d). Stress and Burnout. Retrieved from https://www.practitionerhealth.nhs.uk/stress-and-burnout
Perry, B., Toffner, G., Merrick, T., & Dalton, J. (2011). An exploration of the experience of compassion fatigue in clinical oncology nurses. Canadian Oncology Nursing Journal/Revue Canadienne de Soins Infirmiers en Encologie, 21(2), 91–97.
Rothschild, B. (2006). Help for the helper: The psychophysiology of compassion fatigue and vicarious trauma. W. W. Norton.
Sprang, G., Clark, J. J., & Whitt-Woosley, A. (2007). Compassion fatigue, compassion satisfaction, and burnout: Factors impacting a professional’s quality of life. Journal of Loss and Trauma, 12(3), 259–280.
Stamm, B. H. (2002). Measuring compassion satisfaction as well as fatigue: Developmental history of the Compassion Satisfaction and Fatigue Test. In C. R. Figley (Ed.), Treating compassion fatigue (pp. 107–119). Brunner-Routledge.
Stamm, B. H. (2010). The concise manual for the professional quality of life scale (2nd ed.). ProQOL.org.
Stamm, B. H. (2012). Helping the helpers: Compassion satisfaction and compassion fatigue in self-care, management, and policy. In A.D. Kirkwood & B.H. Stamm (Eds.), Resources for community suicide prevention (pp. 1–4). Idaho State University.
Thieleman, K., & Cacciatore, J. (2014). Witness to suffering: Mindfulness and compassion fatigue among traumatic bereavement volunteers and professionals. Social Work, 59(1), 34–41.
About the author
Dr. Helen Brown is a freelance writer with a Ph.D. in Psychology and MSc in Organizational Psychology. She has a varied background working in mental health and wellbeing research and is passionate about all things psychological. As well as writing about many psychology and health topics, Helen loves to scribble away at fictional stories and screenplays too. You can usually find her in the countryside just south of Bristol, UK.
How useful was this article to you?
Not useful at all
Very useful
Share this article:
Article feedback
Comments
What our readers think
João Leite
on June 23, 2023 at 12:57
Thank you for sharing your article. Recent research from Tania Singer has shown that there is no such thing as Compassion Fatigue. You don’t get tired of being compassionate. You get “emphatic distress”. She has shown that empathy is not pro-social, that why we can get emphatic distress.
This article above should be reviewed and corrected
Thank you for mentioning Tania Singer’s research which differentiates between empathic distress and compassion.
It’s important to acknowledge that “compassion fatigue” is a term historically used, particularly in healthcare, to describe emotional exhaustion from exposure to suffering. Singer’s research suggests that this term might be a misnomer, as it could be more closely related to empathy than compassion.
In light of this, our article could definitely benefit from incorporating or at least acknowledging these distinctions. It’s essential to adapt language and concepts as our understanding evolves. Thanks for bringing this to our attention.
Really insightful and useful article Helen, thank you. As a vet for 28 yrs and now a coach I hadn’t really stopped to look at compassion fatigue but all of it rings true. Times when your tank feels empty. Decisions to step away and recharge for long periods. Reliance on ways to relax like alcohol. Finally choosing to move away from a career that has both given and taken continuously, I get to find my joy in coaching others with a strong focus on positive psychology.
Hello, I am an Office Manager in a Non-helper profession office. I have employees with mental and physical health issues and I am shocked to say, I believe I have compassion fatigue! With so many issues affecting these employees’, their work, our overall work environment and levels, and the continuing nature of all of these, I find I don’t want to listen, or even hear about these issues, to the point of avoidance (not appropriate)! What happened to my empathy? As we come out of the pandemic, what advice and resources are available for us “regular” office workers dealing with compassion fatigue and burnout? Thank you for any assistance.
Nicole Celestine, Ph.D.
on October 6, 2021 at 08:38
Hi Tracy,
I’m sorry to hear you’re experiencing compassion fatigue. I’m sure you’ll agree there are a lot of people in need at the moment, so it’s little wonder the need for empathy is spreading well beyond the typical ‘helping’ professions.
My main suggestion would be to see whether you can engage the people above you to request structural support or an intervention for your staff. If people are coming forward needing support, this may be flowing on to affect their ability to perform, suggesting there’s a likely business case for investing in some support, thereby taking some load off you. You can read more re: this business case in this excellent report by Attridge (2008) and article by Pescund et al. (2015).
For you personally — well done on recognizing that your capacities are being stretched! For a range of suggestions to look after yourself, take a look at our dedicated article for ideas.
 Are you in a caring profession? If so, do you ever feel preoccupied with the suffering of the people you work with?
Are you in a caring profession? If so, do you ever feel preoccupied with the suffering of the people you work with? There are two components to compassion fatigue: secondary traumatic stress and burnout.
There are two components to compassion fatigue: secondary traumatic stress and burnout.
 Anyone in a helping role could develop compassion fatigue, particularly if your compassion satisfaction is dwindling or you’re not getting enough support at work.
Anyone in a helping role could develop compassion fatigue, particularly if your compassion satisfaction is dwindling or you’re not getting enough support at work.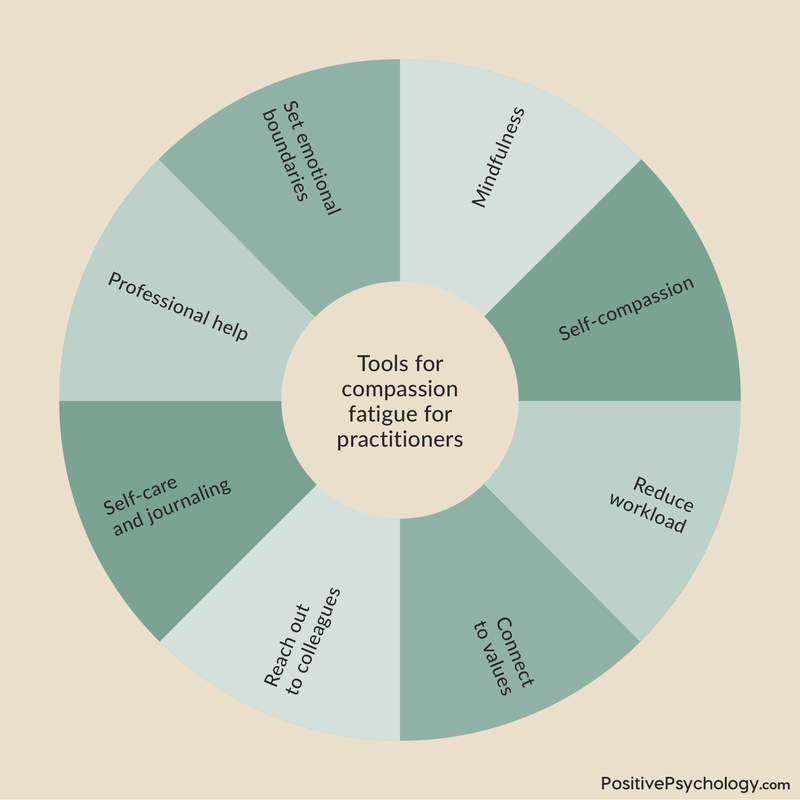
 We are vulnerable to secondary traumatic stress (compassion fatigue) and vicarious traumatization when working with trauma survivors (Jenkins & Baird, 2002).
We are vulnerable to secondary traumatic stress (compassion fatigue) and vicarious traumatization when working with trauma survivors (Jenkins & Baird, 2002).





What our readers think
Thank you for sharing your article. Recent research from Tania Singer has shown that there is no such thing as Compassion Fatigue. You don’t get tired of being compassionate. You get “emphatic distress”. She has shown that empathy is not pro-social, that why we can get emphatic distress.
This article above should be reviewed and corrected
Hi João,
Thank you for mentioning Tania Singer’s research which differentiates between empathic distress and compassion.
It’s important to acknowledge that “compassion fatigue” is a term historically used, particularly in healthcare, to describe emotional exhaustion from exposure to suffering. Singer’s research suggests that this term might be a misnomer, as it could be more closely related to empathy than compassion.
In light of this, our article could definitely benefit from incorporating or at least acknowledging these distinctions. It’s essential to adapt language and concepts as our understanding evolves. Thanks for bringing this to our attention.
Kind regards,
Julia | Community Manager
Really insightful and useful article Helen, thank you. As a vet for 28 yrs and now a coach I hadn’t really stopped to look at compassion fatigue but all of it rings true. Times when your tank feels empty. Decisions to step away and recharge for long periods. Reliance on ways to relax like alcohol. Finally choosing to move away from a career that has both given and taken continuously, I get to find my joy in coaching others with a strong focus on positive psychology.
Dr. Helen Brown, that’s awesome information.
beautiful article. thank you.
Hello, I am an Office Manager in a Non-helper profession office. I have employees with mental and physical health issues and I am shocked to say, I believe I have compassion fatigue! With so many issues affecting these employees’, their work, our overall work environment and levels, and the continuing nature of all of these, I find I don’t want to listen, or even hear about these issues, to the point of avoidance (not appropriate)! What happened to my empathy? As we come out of the pandemic, what advice and resources are available for us “regular” office workers dealing with compassion fatigue and burnout? Thank you for any assistance.
Hi Tracy,
I’m sorry to hear you’re experiencing compassion fatigue. I’m sure you’ll agree there are a lot of people in need at the moment, so it’s little wonder the need for empathy is spreading well beyond the typical ‘helping’ professions.
My main suggestion would be to see whether you can engage the people above you to request structural support or an intervention for your staff. If people are coming forward needing support, this may be flowing on to affect their ability to perform, suggesting there’s a likely business case for investing in some support, thereby taking some load off you. You can read more re: this business case in this excellent report by Attridge (2008) and article by Pescund et al. (2015).
For you personally — well done on recognizing that your capacities are being stretched! For a range of suggestions to look after yourself, take a look at our dedicated article for ideas.
I hope this helps, and best of luck!
– Nicole | Community Manager